How is Melanoma Different From Basal Cell Carcinoma?


Melanoma and basal cell carcinoma differ significantly in their aggressiveness, appearance, and treatment approaches. While basal cell carcinoma grows slowly and rarely spreads, melanoma can metastasize quickly and requires immediate intervention. Hazany Derm provides comprehensive diagnosis and treatment for both skin cancer types.
Skin cancer represents one of the most common forms of cancer worldwide, with millions of new cases diagnosed each year. Among the various types of skin cancer, melanoma and basal cell carcinoma stand out as two of the most frequently encountered forms, yet they differ dramatically in their characteristics, behavior, and treatment requirements. Understanding these differences is crucial for early detection, proper treatment, and optimal patient outcomes.
The distinction between melanoma and basal cell carcinoma extends far beyond their names, encompassing fundamental differences in their cellular origin, growth patterns, and potential for spreading throughout the body. Basal cell carcinoma arises from the basal cells in the deepest layer of the epidermis, while melanoma develops from melanocytes, the pigment-producing cells found in the skin. These cellular origins contribute to vastly different clinical presentations and treatment approaches that patients and healthcare providers must understand.
At Hazany Derm, patients frequently seek clarification about these two skin cancer types, particularly when they notice new or changing lesions on their skin. The ability to recognize the key differences between melanoma and basal cell carcinoma can be life-saving, as early detection and treatment significantly improve outcomes for both conditions. This comprehensive guide explores the critical distinctions between these skin cancers, helping patients make informed decisions about their dermatological health.
Understanding Basal Cell Carcinoma: The Most Common Skin Cancer
Basal cell carcinoma represents approximately 80% of all skin cancer diagnoses, making it the most prevalent form of skin cancer in the United States and worldwide. This type of cancer develops in the basal cell layer of the epidermis, typically in areas that receive frequent sun exposure such as the face, neck, arms, and hands. Despite its high incidence rate, basal cell carcinoma generally exhibits slow growth patterns and rarely metastasizes to other parts of the body.
The development of basal cell carcinoma is strongly linked to cumulative ultraviolet radiation exposure over a person's lifetime, though genetic factors and certain medical conditions can also contribute to its formation. Individuals with fair skin, light-colored eyes, and a history of frequent sunburns face elevated risks for developing this skin cancer. Advanced age, male gender, and immunosuppression further increase the likelihood of basal cell carcinoma development.
Dr. Salar Hazany frequently emphasizes that while basal cell carcinoma is less aggressive than melanoma, it still requires prompt medical attention and appropriate treatment. Left untreated, these cancers can grow larger and deeper, potentially causing significant tissue damage and disfigurement. The slow growth rate of basal cell carcinoma can sometimes lead patients to delay seeking treatment, mistakenly believing the lesion is benign or will resolve on its own.
The clinical presentation of basal cell carcinoma varies considerably, but several characteristic features help distinguish it from other skin lesions:
- Pearl-like appearance: Many basal cell carcinomas present as small, shiny, pearl-like bumps with visible blood vessels running through them
- Central ulceration: Advanced lesions may develop a central crater or ulcer that bleeds easily and fails to heal properly
- Rolled borders: The edges of basal cell carcinomas often appear rolled or raised, creating a distinctive border around the lesion
- Pigmentation variations: Some basal cell carcinomas may appear brown, black, or blue, though most are pink or flesh-colored
Treatment options for basal cell carcinoma depend on factors such as tumor size, location, patient age, and overall health status. Mohs micrographic surgery represents the gold standard for many basal cell carcinomas, particularly those located in cosmetically sensitive areas or recurrent tumors. This precise surgical technique removes cancer cells layer by layer while preserving as much healthy tissue as possible, resulting in cure rates exceeding 99% for primary tumors.
Alternative treatment approaches include traditional surgical excision, electrodesiccation and curettage, cryotherapy, and topical medications for superficial lesions. Hazany Derm offers comprehensive treatment options tailored to each patient's specific needs and circumstances. The choice of treatment method considers not only the clinical characteristics of the tumor but also the patient's preferences, lifestyle, and cosmetic concerns.
Melanoma: The Deadliest Form of Skin Cancer
Melanoma accounts for only about 1% of all skin cancer cases but is responsible for the vast majority of skin cancer-related deaths. This aggressive form of skin cancer develops from melanocytes, the cells responsible for producing melanin, the pigment that gives skin its color. Unlike basal cell carcinoma, melanoma has a strong tendency to metastasize, spreading to lymph nodes and distant organs if not detected and treated early.
The incidence of melanoma has been steadily increasing over the past several decades, particularly among younger populations. While sun exposure remains a significant risk factor, melanoma can develop anywhere on the body, including areas that receive minimal sun exposure such as the palms, soles of feet, and under fingernails. Genetic predisposition plays a more prominent role in melanoma development compared to basal cell carcinoma, with family history and inherited gene mutations significantly increasing risk.
Early detection of melanoma is absolutely critical, as the prognosis depends heavily on the thickness of the tumor at the time of diagnosis. When caught in its earliest stages, melanoma has an excellent prognosis with five-year survival rates exceeding 95%. However, once melanoma spreads to regional lymph nodes or distant sites, survival rates drop dramatically, underscoring the importance of regular skin examinations and prompt evaluation of suspicious lesions.
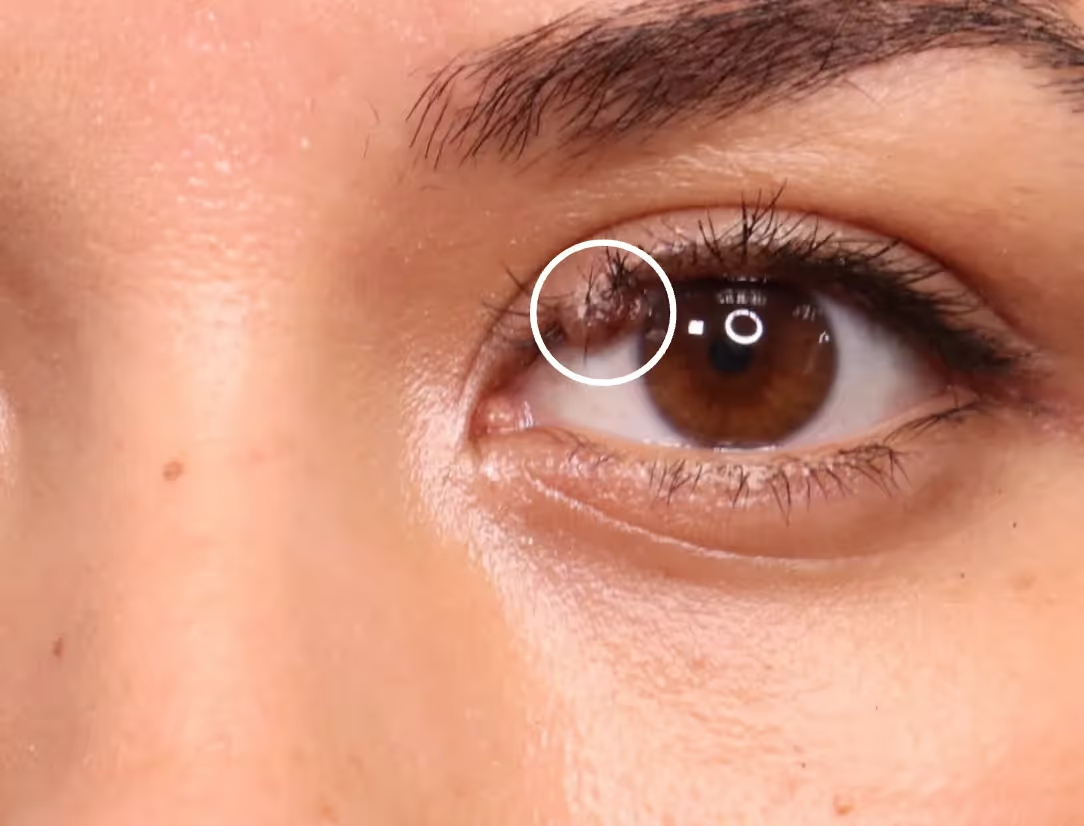
The ABCDE criteria provide an effective framework for identifying potentially malignant melanomas:
- Asymmetry: One half of the lesion does not match the other half in shape, color, or texture
- Border irregularity: The edges of the lesion are uneven, scalloped, or poorly defined rather than smooth and regular
- Color variation: Multiple colors within a single lesion, including shades of brown, black, red, white, or blue
- Diameter changes: Lesions larger than 6 millimeters (about the size of a pencil eraser) or any mole that is growing in size
Treatment of melanoma requires a multidisciplinary approach that may involve dermatologists, surgical oncologists, medical oncologists, and radiation oncologists depending on the stage and extent of the disease. Surgical excision remains the primary treatment for localized melanoma, with wider excision margins compared to other skin cancers to ensure complete removal of cancer cells. Sentinel lymph node biopsy may be recommended for intermediate-thickness melanomas to determine if the cancer has spread to nearby lymph nodes.
For advanced melanoma cases, treatment options have expanded dramatically in recent years with the development of targeted therapy and immunotherapy approaches. These newer treatments have revolutionized melanoma care, offering hope for patients with metastatic disease who previously had limited treatment options. Hazany Derm works closely with oncology specialists to ensure patients receive comprehensive, coordinated care throughout their treatment journey.
Key Differences in Diagnosis, Treatment, and Prognosis
The diagnostic approach for melanoma and basal cell carcinoma shares some similarities but differs in important ways that reflect the distinct characteristics of each cancer type. Both conditions require careful visual examination, often enhanced by dermoscopy, a specialized magnifying tool that allows dermatologists to examine skin lesions in greater detail. However, the urgency and extent of diagnostic workup vary significantly between these two skin cancer types.
For suspected basal cell carcinoma, the diagnostic process typically involves a straightforward biopsy followed by histopathological examination to confirm the diagnosis and determine the specific subtype. Additional staging studies are rarely necessary given the low metastatic potential of basal cell carcinoma. The focus remains on local treatment planning and ensuring complete removal of the tumor with appropriate surgical margins.
Melanoma diagnosis, conversely, requires more extensive evaluation once the initial biopsy confirms the presence of malignant melanoma. Staging studies may include imaging studies such as CT scans, PET scans, or MRI to determine if the cancer has spread beyond the primary site. Blood tests, including lactate dehydrogenase levels, may provide additional prognostic information for advanced cases. Dr. Hazany emphasizes that the thoroughness of initial staging directly impacts treatment planning and long-term outcomes for melanoma patients.
Several critical factors distinguish the diagnostic and prognostic features of these skin cancers:
- Metastatic potential: Basal cell carcinoma rarely spreads beyond the local area, while melanoma frequently metastasizes to lymph nodes and distant organs
- Growth rate: Basal cell carcinomas typically grow slowly over months to years, whereas melanomas can change rapidly over weeks to months
- Surgical margins: Melanoma requires wider surgical excision margins compared to basal cell carcinoma due to its greater propensity for local spread
- Follow-up requirements: Melanoma patients need more intensive long-term surveillance with regular imaging studies and laboratory tests
The treatment philosophy for basal cell carcinoma centers on achieving complete local control while minimizing functional and cosmetic impact. Since these cancers rarely spread beyond their site of origin, successful local treatment essentially cures the patient. Treatment decisions focus on selecting the most appropriate technique based on tumor characteristics, location, and patient factors. Reconstruction considerations play an important role, particularly for lesions in cosmetically sensitive areas.
Melanoma treatment requires a more comprehensive approach that addresses both local control and systemic disease prevention or treatment. Even early-stage melanomas require careful surgical planning with appropriate margins and consideration for sentinel lymph node evaluation. The treatment team must balance the need for adequate cancer control with functional and cosmetic outcomes, recognizing that melanoma patients may require additional procedures and long-term surveillance regardless of initial treatment success.
Frequently Asked Questions
What are the main visual differences between melanoma and basal cell carcinoma?
Basal cell carcinomas typically appear as shiny, pearl-like bumps with visible blood vessels, often developing a central ulcer with rolled borders. They're usually pink or flesh-colored, though some may have brown or black areas. Melanomas, in contrast, are characterized by the ABCDE criteria: asymmetry, irregular borders, color variation within the lesion, diameter larger than 6mm, and evolution or changes over time. Melanomas often display multiple colors including brown, black, red, white, or blue within a single lesion. Dr. Salar Hazany emphasizes that any changing or unusual skin lesion should be evaluated promptly, as early detection significantly impacts treatment outcomes for both cancer types.
Which type of skin cancer spreads more easily to other parts of the body?
Melanoma has a significantly higher tendency to metastasize compared to basal cell carcinoma. While basal cell carcinomas grow slowly and rarely spread beyond their original location, melanomas can quickly spread to lymph nodes and distant organs like the liver, lungs, brain, and bones. This metastatic potential makes melanoma far more dangerous despite being much less common than basal cell carcinoma. Hazany Derm stresses the importance of immediate evaluation for any suspicious pigmented lesions, as melanoma's prognosis depends heavily on catching it before it spreads. Early-stage melanoma has excellent survival rates, but once it metastasizes, treatment becomes much more complex and challenging.
How do treatment approaches differ between these two skin cancers?
Treatment approaches vary significantly between melanoma and basal cell carcinoma due to their different behaviors and risks. Basal cell carcinomas can often be treated with various methods including Mohs surgery, standard excision, electrodesiccation and curettage, or even topical treatments for superficial types. The focus is primarily on complete local removal with good cosmetic results. Melanoma treatment requires wider surgical margins and may involve sentinel lymph node biopsy to check for spread. Advanced melanomas may need additional treatments like immunotherapy or targeted therapy. The team at Hazany Derm develops individualized treatment plans considering the specific characteristics of each cancer type, tumor stage, location, and patient factors.
What are the survival rates for melanoma versus basal cell carcinoma?
The survival rates differ dramatically between these two skin cancer types. Basal cell carcinoma has an excellent prognosis with cure rates approaching 100% when properly treated, as it rarely spreads to other parts of the body. Deaths from basal cell carcinoma are extremely rare and usually occur only in cases of severe neglect or in immunocompromised patients. Melanoma survival rates depend heavily on the stage at diagnosis. Early-stage melanoma (confined to the skin) has five-year survival rates exceeding 95%, but this drops significantly once the cancer spreads to lymph nodes or distant organs. Dr. Hazany emphasizes that early detection is crucial for melanoma, as the difference between early and late-stage diagnosis can be life-determining.
Which type of skin cancer is more common, and who is at higher risk?
Basal cell carcinoma is far more common, accounting for approximately 80% of all skin cancer diagnoses, while melanoma represents only about 1% of skin cancers. However, melanoma causes the majority of skin cancer deaths despite its lower incidence. Risk factors overlap significantly between both types, including fair skin, excessive sun exposure, history of sunburns, and advancing age. Men are at higher risk for basal cell carcinoma, while melanoma affects both sexes more equally and can occur at younger ages. Genetic factors play a more prominent role in melanoma, with family history and inherited mutations significantly increasing risk. Hazany Derm specialists recommend regular skin checks for all patients, particularly those with multiple risk factors or concerning family histories.
How quickly do these cancers typically develop and change?
The growth patterns of melanoma and basal cell carcinoma differ significantly in terms of speed and behavior. Basal cell carcinomas typically develop slowly over months to years, gradually growing larger and sometimes developing central ulceration. Patients may notice these lesions remaining relatively stable for extended periods before seeking treatment. Melanomas, however, can change rapidly over weeks to months, which is why the "E" for evolution in the ABCDE criteria is so important. Melanomas may quickly change in size, shape, color, or texture, and new symptoms like bleeding, itching, or tenderness may develop. Dr. Salar Hazany advises patients to monitor their skin regularly and report any rapidly changing lesions immediately, as the speed of change often correlates with the aggressiveness of the cancer.
What follow-up care is needed after treatment for each type?
Follow-up care requirements differ substantially between melanoma and basal cell carcinoma due to their distinct recurrence risks and metastatic potential. After successful basal cell carcinoma treatment, patients typically need regular skin examinations to monitor for new skin cancers and check the treatment site for any signs of local recurrence. These check-ups are usually scheduled every six to twelve months initially, then annually. Melanoma patients require more intensive surveillance including regular physical examinations, lymph node checks, and sometimes imaging studies or blood tests depending on the original tumor thickness and stage. The Hazany Derm clinic provides comprehensive follow-up care tailored to each patient's specific needs, ensuring appropriate monitoring while avoiding unnecessary anxiety or over-testing.
Can these skin cancers be prevented, and what screening is recommended?
Prevention strategies are similar for both melanoma and basal cell carcinoma, focusing primarily on sun protection and early detection. Daily use of broad-spectrum sunscreen with SPF 30 or higher, protective clothing, seeking shade during peak sun hours, and avoiding tanning beds significantly reduce risk for both cancer types. Regular self-skin examinations help identify new or changing lesions early, while professional skin examinations allow for expert evaluation of suspicious areas. The frequency of professional screenings depends on individual risk factors, with high-risk patients needing annual or even more frequent examinations. The experts at Hazany Derm recommend that all adults perform monthly self-examinations and schedule professional skin checks based on their risk profile, personal history, and family history of skin cancer.