















Types of Active Acne

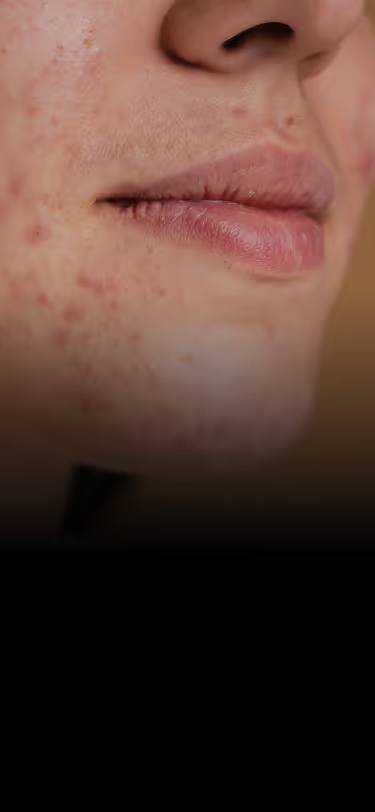
Whiteheads & Blackheads
Comedonal acne develops when excess oil, dead skin, and debris clogs your pores. Comedonal acne is a light or mild form of acne that is either open (i.e., a blackhead) or closed by a thin layer of skin (i.e., a whitehead). Blackheads typically have a darker appearance due to oxygen exposure. Topical spot treatments are effective for comedonal acne. However, comedonal acne that penetrates the skin more deeply might require extraction or another minimally invasive treatment.

Pustules & Papules
Bacteria in the contents of a clogged pore trigger an immune response and causes inflammatory acne. Inflammatory acne is mild to severe. There are two main types of inflammatory acne: pustules and papules. Pustules are red, pus-filled bumps that have a white head. Papules are red bumps that do not have a white head. Common treatments include antibiotics, topical creams, oral medications, and minimally invasive surgery for more persistent inflammatory acne

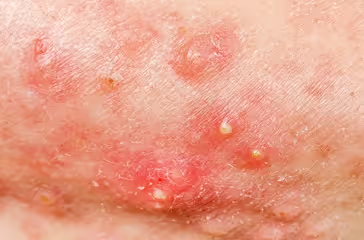
Nodules & Cysts
Nodulocystic acne is a more severe type of inflammatory acne that develops in the deeper layers of skin, presenting a risk for scarring and skin discoloration. Therefore, nodulocystic acne often requires expert treatment. Nodulocystic acne treatment might include topical medications, oral medications, extraction, laser treatment, or other treatments. There are two types of nodulocystic acne: cystic acne and nodular acne.
Cystic acne appears as large, pus-filled lesions that look like pustules. Cystic acne, like pustules, forms a white head. Unlike pustules, cystic lesions are larger and more painful. Nodular acne lesions do not form a white head. Nodular acne forms when debris clogs and irritates skin pores in the deeper layers of the skin. Sometimes, hair follicle walls rupture, allowing debris to contaminate the skin pore, prompting an inflammatory response, and subsequently creating acne nodules.
Active Acne & Scarring Specialist in Los Angeles
Are you looking for the best acne and acne scar treatment in Los Angeles? Dr. Hazany has devoted much of his medical career to understanding acne and acne scarring treatment intricacies. Dr. Hazany specializes in face, back and shoulder acne treatment, in addition to acne outbreaks on other parts of the body.
He empathizes with the emotional distress that his patients experience with acne and acne scarring. Dr. Hazany can help you overcome your acne and acne scarring and restore your self-confidence.






Frequently Asked Questions
Understanding different acne types and their characteristics helps determine appropriate treatment for clear skin.
What is the difference between inflammatory and non-inflammatory acne?
Non-inflammatory acne (comedonal acne) consists of blackheads and whiteheads without redness or swelling. These form when follicles become clogged with sebum and dead skin but without significant bacterial colonization or immune response. Blackheads (open comedones) appear dark due to oxidation of the clog contents, not dirt. Whiteheads (closed comedones) remain beneath the skin surface. Non-inflammatory acne is generally less painful and doesn't scar. Topical retinoids and exfoliating treatments work well for comedonal acne. Inflammatory acne involves the body's immune response to bacteria or follicular rupture, causing redness, swelling, and sometimes pain. Papules, pustules, nodules, and cysts are inflammatory lesions. Inflammatory acne poses greater scarring risk and requires more aggressive treatment. Many patients have both types simultaneously, requiring combination therapy. Dr. Hazany assesses lesion types to determine the appropriate treatment balance.
What is cystic acne and why is it so severe?
Cystic acne involves deep, severe inflammatory lesions that extend into the dermis (deeper skin layer). Cysts feel firm to hard, are painful, and are the largest acne lesions possible. They form when a clogged follicle ruptures and the body's inflammatory response traps pus deep in the skin. Unlike pustules which contain visible pus at the surface, cysts are deep and closed. Cystic acne causes significant pain, often persisting for weeks. The extensive inflammation and depth cause damage to collagen structure, making cystic acne the most likely type to scar. Cystic acne can leave permanent scars even after healing. The severe inflammation also often causes postinflammatory hyperpigmentation, especially in darker skin types. Cystic acne requires aggressive treatment, often including oral medications like antibiotics or isotretinoin. Dr. Hazany prioritizes early, aggressive treatment of cystic acne to prevent the severe scarring this type causes.
What causes hormonal acne and how is it different from other acne?
Hormonal acne is driven by hormonal fluctuations affecting sebum production and follicular function. In women, hormonal acne typically worsens before menstruation due to progesterone surges. Hormonal acne often develops in women in their 20s-40s who didn't have severe acne as teenagers. The pattern of jawline, neck, and chin acne is characteristic of hormonal breakouts. Hormonal acne tends to be moderately inflammatory with papules and pustules rather than comedones. Unlike comedonal acne that responds well to retinoids, hormonal acne benefits from hormonal treatment. Oral contraceptives containing specific progestin types can improve hormonal acne. Spironolactone, an androgen-blocking medication, treats hormone-driven acne. Antibiotics provide symptomatic improvement while hormonal treatments address the root cause. Dr. Hazany evaluates acne patterns and timing to identify hormonal components. Treatment often combines hormonal therapy with topical or oral antimicrobial agents for comprehensive control.
What is acne rosacea and how does it differ from common acne?
Acne rosacea is sometimes called rosacea with acneiform lesions; it's distinct from common acne (acne vulgaris) despite superficial similarities. Rosacea causes facial redness and visible blood vessels (telangiectasia) along with pustules and sometimes papules. Unlike acne vulgaris, rosacea doesn't involve comedones or blackheads. Rosacea is more common in fair-skinned individuals and typically appears in middle age. Common acne predominantly affects adolescents and can occur at any age. Rosacea is triggered by heat, spicy foods, alcohol, and emotional stress. Common acne relates to sebum, bacteria, and inflammation. The treatment differs—rosacea responds to anti-inflammatory treatments and antibiotics but not retinoids or stronger acne medications. Oral antibiotics at sub-antimicrobial doses treat rosacea's inflammation. Laser treatments can address rosacea's vascular component. Misdiagnosing rosacea as acne leads to inappropriate treatment. Dr. Hazany carefully distinguishes between conditions to provide appropriate care.
What is fungal acne and how is it different from bacterial acne?
Fungal acne, also called malassezia folliculitis, is caused by yeast (Malassezia) colonization of follicles rather than bacteria. Fungal acne appears as small, uniform pustules, often on the chest, shoulders, or back. Unlike typical acne, fungal acne doesn't respond to antibiotics or standard acne medications. Fungal acne can be itchy or tender, distinguishing it from bacterial acne. The condition is more common in warm, humid climates and in people with oily skin. Certain activities like wearing tight clothes or sweating exacerbate fungal acne. Diagnosis requires clinical observation and sometimes microscopy or culture. Treatment involves antifungal medications like ketoconazole or selenium sulfide washes. Oral antifungals may be necessary for extensive cases. Distinguishing fungal acne from bacterial acne is important because standard acne treatments won't help. Dr. Hazany considers fungal acne in patients whose acne isn't responding to appropriate antibacterial treatment.
What is drug-induced acne and what causes it?
Drug-induced acne is acneiform eruptions caused by certain medications rather than typical acne causes. Corticosteroids are the most common culprits, inducing acne-like lesions through inflammatory pathways. Lithium (used for bipolar disorder), certain vitamins, and anticonvulsants can cause acne. Anabolic steroids used for bodybuilding cause severe acne through hormonal effects. Some antibiotics can promote fungal or bacterial overgrowth leading to acne. Topical products with occlusive ingredients can trigger acne. Drug-induced acne appears differently than typical acne—lesions are often uniform and monomorphic. The timing usually correlates with medication initiation. Management involves identifying the causative medication and considering alternatives if possible. If stopping the medication isn't feasible, treating acne symptomatically is necessary. Recognizing drug-induced acne prevents unnecessary dermatologic treatment and points toward the underlying cause. Dr. Hazany takes thorough medication histories to identify potential medication-acne relationships.
