















Types of Acne Scarring



Atrophic Acne Scars
Acne lesions that heal below the top layers of skin create atrophic scars, which appear as depressions or indentations in the skin. While different types of active acne cause atrophic scarring, severe cystic acne is the most common cause. The severity of atrophic scarring may vary depending on the severity of a person's acne history.
Atrophic acne scars have three different subtypes. The most common types of atrophic scars are:
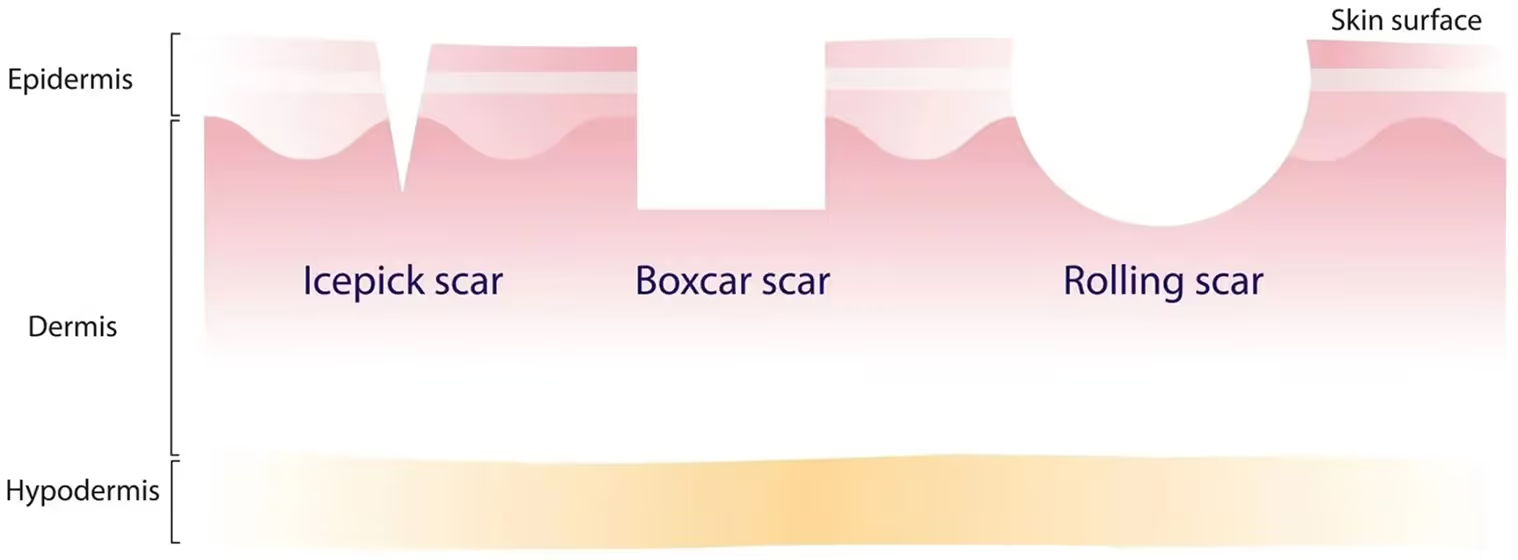
- Ice pick
- Boxcar
- Rolling
Atrophic scars result from the loss of collagen during the skin’s inflammatory healing process. The localized degradation of collagen and subcutaneous fat causes the affected area to dip below the level of healthy skin tissue. The type of atrophic scar that tends to form varies for each person. Here are the most common causes ofatrophic scarring:
- Chicken pox
- Shingles
- Vaccine shot
- Insect/spider bite
- Acne
- Trauma


Boxcar Scars
Boxcar scars are typically round or square depressions, with sharp demarcations and vertical walls. Boxcar scars vary in depth, but the base of boxcar scars is usually flat and the same size as the scar's opening at the skin's surface. This type of scarring typically forms in areas where the skin is relatively thicker, such as the lower cheeks and jaw.
Although boxcar scars can be treated with a variety of procedures, many of them, including laser, dermabrasion, and microneedling, work superficially and are ineffective for deeper scars. At our clinic, subcision, punch excision, and collagen stimulators are the most effective and long-lasting treatment options for especially deep boxcar scars. We will perform a thorough evaluation of each of your boxcar scars to customize your treatment plan.


Ice Pick Scars
Ice pick scars are more narrow, smaller indentations that extend deep into the skin's layers (into the dermis, and even into the subcutaneous tissue). The scar's opening is wider and tapers off at the base, creating an ice pick-like shape. Because icepick scars penetrate the skin's deeper layers, they typically require more aggressive acne scarring procedures. Ice pick scars are common on the cheek area. They can also appear on the forehead and nose.
In general, ice pick scars have repeatedly been shown to respond well to phenol CROSS, our frontline treatment method. However, patients with more severe ice pick scars may benefit more from punch excision, a process in which a small “cookie-cutter” tool is used to punch out the ice pick scar. In this manner, we ensure that the scar is removed in its entirety, as opposed to other treatments that merely treat the surface.


Rolling Scars
Rolling scars vary in depth and have sloping edges that create a wavy, uneven appearance. These scars develop when fibrous tissue tethers the epidermis to the underlying subcutaneous tissue, creating sloping and wave-like indentations in the skin. Rolling scars are shallow and soft depressions that become more noticeable when skin ages and loses its elasticity. Rolling scars can disappear over time but may require intervention depending on their severity.
Because rolling scars are the softest among the different scar types, they respond the best to subcision followed by collagen stimulation. We will perform a thorough evaluation of your rolling scars to assess their severity and depth to determine what layers will need to be subcised. It is important to manually sever the fibrotic tethers in multiple layers to completely remodel the skin. Any treatments that do not target these tethers will not solve the root cause of rolling scars.
Hypertrophic and Keloid Acne Scars
Different from atrophic scars, hypertrophic scars and keloid scars are types of acne scar overgrowth. Hypertrophic scars are raised scars that do not grow beyond the size of the original acne lesions. In contrast, keloid scars are raised scars that grow beyond the size of the original acne lesions, and appear as if though they "mushroom" out from the location of the lesion.
These scars generally have the following characteristics:
- Shiny luster
- Rubbery texture
- Raised
- Hairless
Hypertrophic and keloid scars are common on the back, chest, jawline, and shoulders. Also, people with darker skin are more likely to develop hypertrophic and keloid scarring.
Keloid scars generally result from injury to the skin, including damage from chickenpox, acne, post-surgical scarring, lacerations, and more. These scars are commonly observed on the ear lobe, chest, shoulder, and upper back. Some individuals are especially prone to developing keloid scars, notably Asian and Black individuals. Keloid scars may start off small in the beginning but can grow noticeably larger over time.
Listed below are common causes for keloid scars:
- Burns
- Surgery
- Piercings
- Chicken pox
- Shingles
- Vaccine shot
- Insect/spider bite
- Acne
- Trauma
- Cuts
Because keloid scars are characterized as overgrowths, Kenalog or steroid injections can be used to reduce the size of the keloid scar. These injections work by breaking the collagen fibers within the scar tissue. Surgical removal of the keloid can also be carefully performed, leaving minimal scars afterwards. Cryotherapy can treat smaller keloids by freezing and killing scar tissue in a controlled manner. Lastly, laser therapy may help improve the color and appearance of keloid scars, although laser therapy alone may not be able to remove the scar tissue entirely.






Frequently Asked Questions
Comprehensive guide to different acne scar types and their specific treatment approaches for optimal improvement.
What is the difference between atrophic and hypertrophic scars?
Atrophic scars (depressed scars) are indentations where skin is lost or collagen is insufficient. Ice-pick, rolling, and boxcar scars are all atrophic types. Atrophic scars are far more common from acne than hypertrophic scars. Hypertrophic scars are raised, thickened scars where excess collagen is deposited. Hypertrophic scars appear red and firm, sometimes itchy. Hypertrophic scars are more common on the back and chest from body acne. Darker skin types are at higher risk for hypertrophic and keloid scarring. Treatment differs between types; atrophic scars benefit from subcision and resurfacing, while hypertrophic scars benefit from flattening treatments. Understanding scar type guides appropriate treatment selection. Dr. Hazany carefully categorizes scars to determine optimal treatment approaches.
What are ice-pick scars and how are they treated?
Ice-pick scars are narrow, deep, sharply demarcated depressions resembling puncture wounds from an ice pick. They're among the most difficult acne scars to treat due to their depth and narrow opening. Ice-pick scars result from the follicle rupturing and deep inflammation destroying significant collagen. The narrow opening makes filling these scars difficult. TCA CROSS is particularly effective for ice-pick scars by chemically resorbing the scar tissue. Laser treatments can improve ice-pick scars but may not completely fill them. Subcision is less effective for ice-pick scars due to their narrow configuration. Dermal fillers can temporarily fill ice-pick scars but require repeated treatments. Combination treatments using TCA CROSS plus laser or subcision produce better results than single treatments. Dr. Hazany has extensive experience treating ice-pick scars and achieves impressive improvements.
What are rolling scars and how are they treated?
Rolling scars are wide, shallow depressions with sloping, rounded edges created by tethering of deeper scar tissue. Rolling scars appear as waviness or undulation in the skin surface. Unlike ice-pick scars which are narrow and deep, rolling scars are broad and relatively shallow. Rolling scars result from collagen loss creating tethering rather than direct tissue loss. Subcision is highly effective for rolling scars by releasing the tethering beneath. Laser treatments improve rolling scars by remodeling the surface and stimulating collagen. Microneedling can improve rolling scars through collagen stimulation. Combination approaches using subcision plus laser produce the best results. Rolling scars often respond remarkably well to appropriate treatment. Dr. Hazany's expertise with subcision produces excellent results for rolling scarring.
What are boxcar scars and how are they treated?
Boxcar scars are relatively broad, rectangular or irregular depressions with sharply defined edges. Boxcar scars resemble pitted skin or small boxcar dents. The sharp edges distinguish boxcar scars from rolling scars. Boxcar scars are created by broader collagen loss compared to ice-pick scars. The sharp edges make boxcar scars noticeable but their relative shallowness compared to ice-pick scars means they often respond well to treatment. Laser treatments are effective for boxcar scars by remodeling the edges and surface. Subcision works for boxcar scars if tethering is contributing. Chemical peels improve boxcar scars through remodeling. Dermal fillers can temporarily fill shallow boxcar scars. Combination approaches produce better results than single treatments. Dr. Hazany tailors treatment to the specific characteristics of each patient's boxcar scars.
What is the difference between postinflammatory erythema and scarring?
Postinflammatory erythema (PIE) is persistent redness after acne lesions heal without true scarring or loss of skin integrity. PIE results from prolonged inflammation and increased blood vessel visibility. PIE eventually resolves on its own, though it may take months to years. True scarring involves permanent changes in skin structure and collagen. Distinguishing PIE from true scars is important for treatment planning. Early appearing redness after acne healing often represents PIE rather than scarring. Sun protection and time often improve PIE without treatment. Laser treatments and other procedures may provide faster improvement of PIE. Many patients misidentify PIE as scarring, leading to concern. Dr. Hazany can distinguish PIE from true scars and provide appropriate reassurance about natural resolution when appropriate.
How does skin type affect acne scarring and treatment?
Skin type significantly influences both scarring tendency and treatment approach. Darker skin types are at higher risk for keloid and hypertrophic scarring compared to fair skin types. Darker skin types also have higher risk of postinflammatory hyperpigmentation complicating scars. Fair skin types more commonly develop atrophic scars. Treatment response differs by skin type; certain lasers work better on lighter skin while others work better on darker skin. Thermal injury risk differs with darker skin types requiring careful technique selection. Chemical peels require different concentrations and timing for different skin types. Dr. Hazany's experience with diverse skin types ensures treatment is appropriately customized. Understanding individual skin characteristics optimizes treatment selection and outcomes
